
It’s coming to the end of another Advent weekend and I am moving towards being caught up with life. Not completely… that will never happen… but I am at least done with everything that has to be finished before the next, and last work week for the year begins in the morning. I am hoping that the tendency of people not to want to go to the doctor continues as I feel in need of some R and R. I am going to get that starting on the 22nd when I can hang up my shingle until January the 8th. I am headed for NYC for a good bit of it- the gang who went to London for New Year’s last year is hitting another cultural capital this year- so if you’re NYC based and want to get together sometime between the 27th and the 3rd, drop me a line. I have made a deliberate decision to do minimal advance planning and scheduling and just let that week happen. Maybe I’ll see some shows. Maybe I’ll sleep fourteen hours a day and read a couple of good books. Maybe I’ll have them lock me in the Metropolitan Museum after hours so I can have a ‘From the Mixed Up Files of Mrs. Basil E. Frankweiler’ moment.
Seven Santas closed this afternoon with the matinee performance and another project has been put to bed. I really quite enjoyed this one. There’s something therapeutic about screaming in another actors face or going from despair to uncontrolled rage to sardonic laughter in about three minutes. Given the triggers written into the script for my character, Red, putting the show to bed is about as apt a metaphor as I could come up with. I’ll miss my other six Santas and Mrs. Claus as it was very much an ensemble show with each of us being an integral part of the structure and staging. All eight of us got along exceedingly well and had a blast working together to create the rather depraved humor of the piece. I won’t have too long to mourn theatrically, however, as my first rehearsal for Into The Woods is tomorrow evening. I finally received the full cast list and it’s very definitely split into the old guard, people with whom I’ve worked many times over the years, and the young uns who are up and coming and whom I am looking forward to getting to know better.
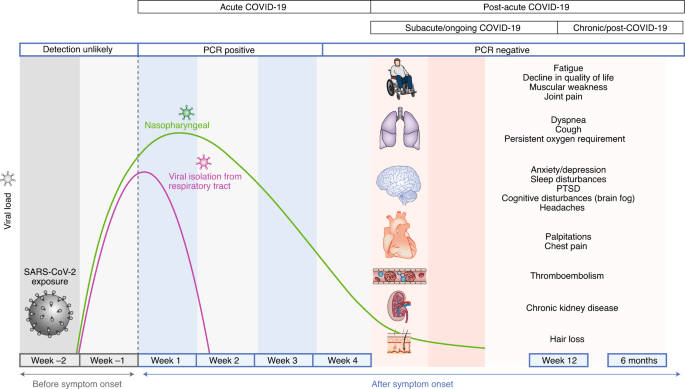
Respiratory illness is definitely continuing to spread locally. There’s been some Covid, but most of it is the crud. I continue to search for good information on what Covid is actually doing these days but the usual fragmentation of public health information that happens when the federal government is not involved in an active emergency situation stymies any easy digesting of the numbers. There’s also the overlay of antivaccine movement noise that tries to interpret issues in ways that favor their worldview whether that’s what the data actually say or not and you have to try to sift through that as well. Hospitalizations and deaths, while up, are not anywhere near where they have been in the past. But as I start to think about it, these are not the most useful metrics for this phase of the disease. Much more useful would be numbers that allow us to track Long Covid or post Covid complications with clotting or heart or neurologic issues in relatively young people that may have enormous bearings on total morbidity and mortality for society as time goes on. No one seems to be counting and reporting any of that in any sort of systematic way. No one can even agree on what Long Covid is and is not.
There are a couple of local physicians whom have set themselves up as specialists in Long Covid and vaccine injury. I imagine there are a few in every community who are seizing on this business opportunity. From what I can tell, they are preying on desperate people with promises based on therapies with no scientific data to back them. And selling all sorts of supplements out of their offices to boot. There’s an old saying in medicine. The A students become medical school faculty, the B students become good doctors, and the C students become millionaires. I was a B. I would not have become med school faculty i I had not chosen a field that was enormously underserved. If you come to me with signs and symptoms of Long Covid, I’m going to tell you what we know (not much), what we don’t know (a lot), and figure out a treatment plan with some rationale that will interdigitate with your other disease processes and who you are. I’m not referring you to a self styled specialist who seems to be motivated by profit.
There was a long article in today’s Washington Post (which I posted elsewhere) about one of the dirty little secrets of American health care – the Assisted Living industry. There are three basic levels of residential senior care – independent where you live as you please but where the community may offer services such as communal dining and housekeeping – assisted where you have staff to help you with things you cannot do for yourself safely such as bathe when you are wobbly on your feet (it gets subdivided in most states into regular and dementia/memory care) – and skilled nursing which provides those who need regular nursing attendance to care for their own bodies or who have major issues such as catheters and feeding tubes.
Most people assume that all of these are licensed and regulated in the same way. They are not. Skilled nursing, as it can be paid for with federal dollars (mainly through a state Medicaid program although Medicare does step in in certain limited situations to help someone get over the hump after illness or injury) is subject to intense federal regulation, similar to that which polices hospitals. There are more rules and regulations on skilled nursing facilities than practically any other industry in the country (including commercial aviation and nuclear power) and the feds have significant powers over a SNF in terms of fines and licensure. They don’t always exert those powers, but that’s another story. The up side is that there are regulatory teeth and the facilities and their operators understand this. The down side is that the RN is more likely to be doing paperwork to ensure better audit scores than actually providing any meaningful patient care.

Assisted living, however, is not regulated at all at the federal level as no federal dollars flow into them. (A state Medicaid program can pay for assisted living if it so chooses, but there are no requirements. This does not happen in Alabama.) It’s entirely up to the states. And the industry lobbies long and hard to prevent federal regulation and to keep state regulation cursory at best. ALF regulation is actually pretty good in Alabama. It’s one of the best states for oversight. As there are minimal public funds going into them, they are pretty much entirely private pay and generally attract the upper classes on the socioeconomic scale. The lower ones handle their elders at home as a fee of $5000-7500 a month is beyond their means.
What do you get for these costs? You will be told, especially for the demented, that you will get 24/7 supervisory care to prevent accident or wandering or any of the other major behavioral issues that make dementia patients difficult at home. They represent a safe alternative to being at home and getting into mischief when a broken brain makes an older adult do things that they believe are entirely correct (they often still think of themselves as healthy vibrant adults not in need of supervision) but which families and the world in general may look upon askance. There are promises of frequent checks, trained staff, nutritious meals etc. And there’s the money that goes into the furnishings in the public areas to instill a sense of security in families.
The Post article takes a deep dive into the thousands of patients that wander away from Assisted Living every year and the hundreds that have died from exposure or other misadventure as they cannot find their way back due to the disorientation that often accompanies dementia. It then goes into the consequences of these events (not much) and how they come to occur (understaffing, under trained staff, an emphasis on collection of monthly fees over actually providing care). And, as the federal government is not involved, when something goes drastically wrong, the legal remedies are somewhat limited. And in many cases, a clause limiting to binding arbitration is part of the admission documents.

I do a little medical legal work on the side. It’s how I get the money I give to local theater companies so don’t judge me too harshly. Doing this sort of thing has allowed me to peek behind the curtain when something has gone wrong and see how the long term care industry operates. It used to be a not for profit sector but no longer. It’s now mainly corporate chains hiding behind cozy local names with multiple interlocking companies used to shield each other from trouble. One company owns the building and another employs the nursing staff and a third runs the kitchen etc. A dogged plaintiff’s lawyer can cut through all of it but it can take years and most families aren’t cut out for the process. But when they are, you can finally get the budget sheets for the kitchen and find out that the allocation for meals per resident is just over four dollars a day. (That’s not the norm – that was something that came up in a case of adult failure to thrive and weight loss where the resident kept complaining to the family about the quality of the food.)
I encourage everyone to seek out the article and read it. Because the issues highlighted are about to get much, much worse with the aging of the Baby Boom. They have yet to really hit the dementia belt but that’s going to change within the next five years. What will those pressures bring? Federal regulation? Unlikely without federal dollars being involved. Improved state regulation? Industry trade groups will be able to outspend concerned citizens at every level. Probably just more sad stories and a decline in the number of existing beds if corporate America feels that the sector is going to become unprofitable. And then there’s the continued issue of lack of staffing. That’s not likely to improve anytime in the near future, especially with the current negative feelings towards immigration. Nursing aide is often the first step on the ladder for new immigrant women.
In the meantime, I am not trying to discourage anyone form using Assisted Living if it’s the appropriate solution to their family’s needs. But Caveat Emptor. Don’t make your decisions based on marketing materials and floral displays in the dining area. Ask around. I’m happy to give my impressions of local senior living communities. I’ve been in most of them, know many hard working and dedicated people who work in them, and listen to what patients and their families have to say about their experiences.
