Time marches on and summer turns to fall. Around here, that means that the humidity has finally left the air and we’re having lovely days of 70s and low 80s that don’t feel like a malfunctioning steam bath and I, at least, don’t mind being out of doors. There’s also a bit of a nip in the air when I walk out the door in the morning and I’ll have to get out my official UAB jacket soon so I don’t develop too many goosebumps in my daily race from one office to another, trying to keep all the professional balls in the air.
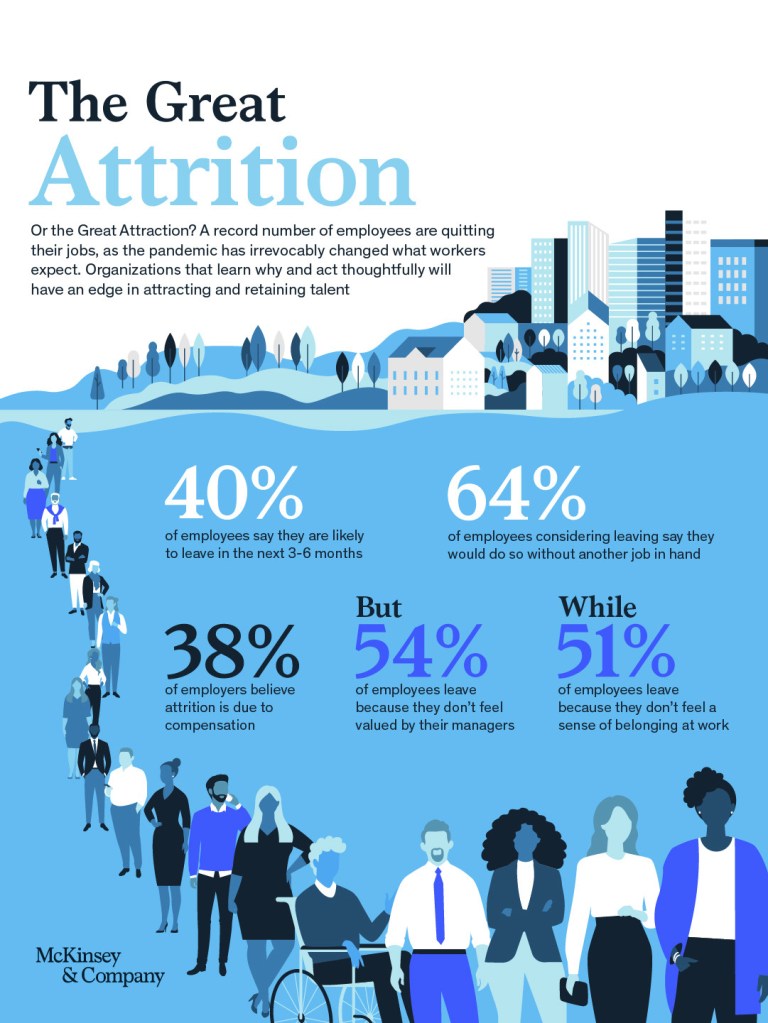
The pandemic has done a number on health care. The effect on my specialty is not one of direct effect. Most of my patients were smart enough to isolate through the worst of it in 2020 and then get vaccinated as soon as they could in 2021. It’s the indirect effects. Disease processes having worsened because of delayed care. Impossibility of getting timely specialty services due to retirements and short staffing. The inability of senior living facilities and other services to meet demand and the endless array of complaints this brings to us from fed up patients and families – as if we had any control. The significant increase in mental health issues, especially anxiety which has led to more and more communications with our offices over relatively minor issues. Phone calls, emails, faxes, notes, complaints all up. Staffing down. One very tired and somewhat exasperated geriatrician caught in the middle. One of these days I will be able to convince the powers that be that for every person who comes through the door providing a billable visit, we hear from another eight or nine people that require some assistance that day (unbillable work and therefore not part of the computations regarding the need to increase staffing). Perhaps I should take an unscheduled vacation and forward all my phone lines and messages to the Dean’s office for a week.
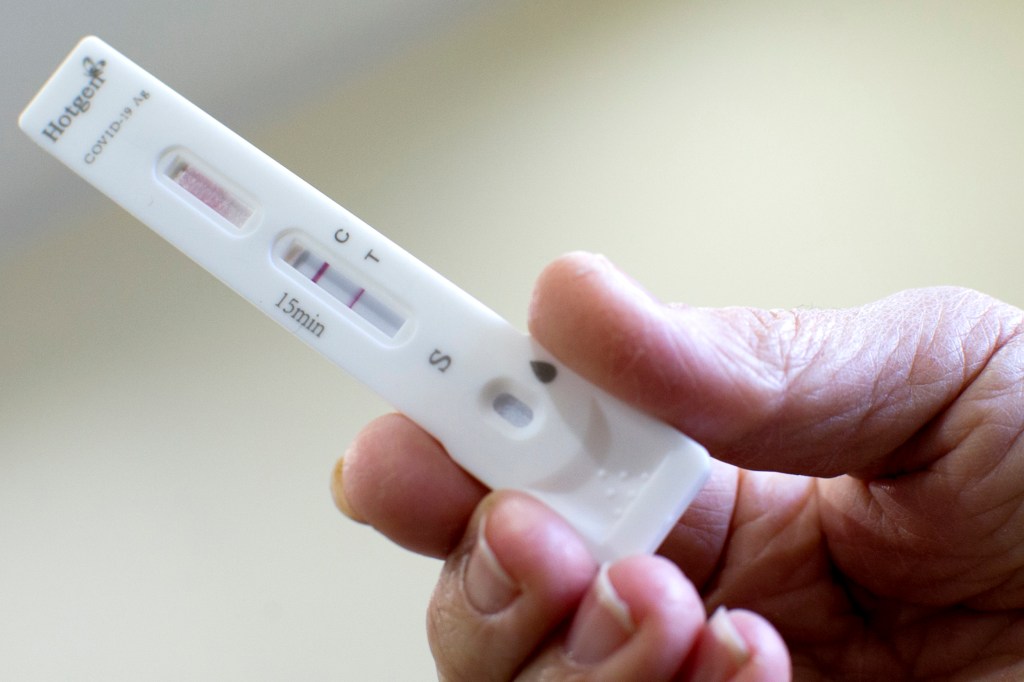
A review of the numbers shows that we’re holding relatively steady at about 400 deaths daily but cases have continued to decline somewhat. I don’t know how much to trust the data in general as so there’s now so much variation in reportage but it looks like the current hot spots are Appalachia, especially Eastern Kentucky and Western Virginia and the Mountain West. I wonder if that’s related to lower vaccination rates in those areas due to political leanings. There’s still a lot of fear in the epidemiologic community that we’re going to go back up again significantly later in the fall as various omicron subvariants continue to spread and because people continue to not take advantage of our best weapon, vaccination.

The new bivalent vaccinations have been out for about a month now with their increased specificity against omicron. Not a lot of folk are taking advantage of them despite widespread availability. It may be due to the collapse of media coverage of Covid in the wake of other stories of national interest and the lead up to the midterm elections. It may be because the populations most likely to take advantage are waiting a bit more to take them a bit later in the fall along with their usual flu shot. It may be that there are a lot of folk like me, who had a mild infection within the last few months and are waiting out their three month post infection window before getting another booster. As more and more data comes in on the bivalent vaccine in populations, it is becoming clear that it provides longer protection, stronger protection, and broader protection allowing the immune system to react positively against new subvariants as they come into being. There’s a lot of reasons to get boosted if you’re over fifty or have an immune system issue or a chronic illness and not a lot of good reasons not to.

The Hallelujah Girls is up on its feet and half way through its glorious four performance run. It’s been a good time. It’s very rare for me to get cast as a romantic comedy lead as I’m a character type so I’m making the best of it as it’s likely to be a while before I get the girl on stage again. It’s not Shakespeare, Sheridan, Shaw or Shaffer, but it’s good fun and audiences are enjoying it and laughing appropriately at the antics of the Southern Belles and Rednecks inhabiting the Spa-Dee-Da day spa in the old church building in Eden Falls, Georgia. Most of the cast are people whom I have not worked with before and it’s been fun getting to know some new and talented folk. After closing on Sunday, I am turning off my theater brain for a few weeks, forgetting my pages of bad grammar dialog, ditching my redneck accent, and taking a few naps. I’m still not recovered from my recent Covid bout and just get tired far too easily. I can tell I’m improving but I keep falling asleep in the passenger seat on house calls or sitting in front of my computer writing notes and haven’t been able to do much outside of work/dress rehearsal/performance all week and the laundry and grocery store are calling.
I don’t have a publication date on Volume II of The Accidental Plague Diaries yet. Stop asking. As soon as it’s set, I’ll make sure everybody knows. There’s still a few more tweaks to make sure it’s all finished and good as it can be. In the meantime, go get your booster if eligible, stay home if you’re sick, and keep your hands washed.