And the proof pages fly by, one by one. I’m now about two thirds of the way through the final proofs of Volume III of The Accidental Plague Diaries and barring something really unfortunate happening this weekend, it will all be signed, sealed, delivered back to the publisher before the end of the month. Then, assuming all goes well in Seattle, I should be able to announce a publication date for late October or early November and then this project, which has been an over arcing theme in my life for the last nearly four years will be done. Unless I have to put significant time into a Kindle edition, an audio edition, and some sort of monologue adaptation. It’s rather odd to think that I’ve spent more time on this than time in high school, college, or medical school. When I do hold Volume III in my hands, I think I’ll have to figure out some sort of valedictory celebration.
UAB has a new social media initiative ‘Humans of UAB’ based on the New York Times series ‘Humans of New York’ which has been running for the last couple of years. For some reason known only to the PR department, they decided that I was a human this month and the piece came out yesterday. I was quite taken with the photograph they took. (It’s my new profile photo) but I’m not sure that UAB truly appreciated the subtext of my remarks. My comments on being human in medicine, on a reread, suggest that to be human and to work within the modern American healthcare industry, one must forever swim upstream, pushing against the way that things are done. And that this gentle refusal to go along to get along, while better for patients, will limit the ability to rise within the system. I’ve certainly seen that play out in my career both with my personal experiences and in watching others battles. And I came to the conclusion a long time ago that I would rather do the right thing and insulate myself somewhat from the system at large than compromise for the sake of a nicer office or a higher salary.
I had a text conversation this morning with an old friend; she has a sister with a complex, chronic autoimmune disease which has led to a lot of interactions with the the health system. She started out with an innocuous enough question. Was I aware of any local primary care physicians who took care of their own patients when they were in the hospital as well as seeing to their outpatient needs. I really didn’t know of any. And then it occurred to me that that was the standard model of care from the turn of the last century and the beginnings of the modern hospital through the 1980s. I was of the last generation of internists who was trained to be able to do both inpatient and outpatient care and who was expected to follow that sort of career path. I finished by residency in 1991, but by 1995-2000 significant economic changes in medicine led to the creation of the inpatient hospitalist who would to the inpatient work leading primary care physicians to focus on outpatient care. This was a major paradigm shift.
Why did this happen? The shift of the system from its not for profit roots to for profit models demanded greater efficiencies from the parts of the system. Having physicians in the hospital to deal immediately with issues and with the more complex medical illnesses that could now be treated with more modern medications and technology rather than the nurses having to track the physician down in his office down the street for new orders allowed a physician to provide services to more patients at once. At the same time, the reimbursements per patient for non technical services, the thought part of medical practice, were being ratcheted down by the system so a primary care physician needed to see more and more visits per work day to keep the funds flowing in the practice to pay themselves and cover their office overhead. The aging of the population and the survival of more and more individuals with chronic illness that would have carried them off a generation or two ago led to more and more demands for good primary care.
Primary care began to involute. More and more medical school graduates decided to avoid it. In my graduating residency class, about half became primary care internists of one stripe or another. Now only about 15% do based on the last national statistics I’ve seen. They become hospitalists (well paid, shift work so no scheduling hassles, basically the same job they were doing as residents so very familiar working conditions) or technical subspecialists with much higher incomes. I can’t say I blame them. If I was looking at putting three or four kids through college and paying for a couple of society weddings, I might make a similar decision but my children have remained safely unborn. This huge gap between supply and demand is what’s led to the rise of the physician assistant and the nurse practitioner. I’d love to see all of my patients every time they come in but I don’t have thirty hours a day nine days a week.
The stresses and strains of the pandemic, with its mass retirements and various shortages of personnel, equipment and supplies, more or less ripped the veneer off the rickety American health system. It’s well known that our system consumes nearly twice the GDP percentage than it does in other wealthy nations and our outcomes are at the bottom of the heap when it comes to the international rankings. 11th out of 11 of the wealthiest nations and 37th out of all countries on the WHO scoreboard, nestled in between Slovenia and Costa Rica. The built in silo between the worlds of inpatient and outpatient, made rigid through various financial systems, makes it very difficult to coordinate care between those worlds. There are some ways around this. Small rural communities still follow the old way of the generalist providing both inpatient and outpatient care but those hospitals are falling like dominoes in recent years due to unsustainable deficit spending. There’s also the concierge model where you can pay a fee to the practice for ‘non-covered by insurance medical services’. That fee brings money in so that the practice doesn’t have to see an enormous number of individuals daily to keep the doors open, allowing the physicians time for longer consultations and time to make hospital rounds (although even then they usually collaborate with hospitalists due to the acuity of most hospitalized patients these days).
Then there are the complications of our new documentation systems known as Electronic Health Records. In theory, an EHR is a very good thing. One integrated health record usable by all so that things won’t fall through the cracks. In practice, however… The systems were created for administrative tasks – big data collection and analysis, QA projects, billing, and other similar things. And administrators working at home for two years had plenty of time to fool around with them and come up with more and more projects of interest. The problem with big data, however, is someone has to collect and enter the data. And that has usually fallen to the person at bedside inpatient (nurse or physician) or in the clinic exam room (same). These systems are now so chock full of boxes to be checked and data points that it’s often very difficult to separate the wheat from the chaff and therefore, as notes grow to six or seven pages of seemingly unrelated datapoints thrown out automatically by the system, more and more of the notes go unread.
My friend, who helps her sister navigate multiple specialists, is meticulous and keeps excellent notes and records regarding her health conditions and provides written copies to physicians of what they need to know. They are dutifully entered in to systems but there is so much there that no one is likely to ever find or read or act on any of this knowledge that has been obtained through years of trial and error. And she has to start over every time a new character enters the stage. My ultimate suggestions – move somewhere where the old system prevails, leave the country for a place with a health system rather than a health industry, or hold your nose and pay a concierge fee. I’m probably going to do that last should I develop health conditions that start to significantly impact my function. And once again, American capitalism creates an unofficial two tiered system.
Another friend contacted me this week about his 101 year old mother resident in a nursing home and how her care keeps falling through the cracks. Not much I can do directly as she is not my patient, but it all boils down to short staffing. The only way for him to effect change is going to be being present as much as possible and demand that the nursing home deliver the care it’s being paid to deliver. He won’t endear himself to the staff, but his mother will do better in the long run. Sometimes you have to be the squeaky wheel. I get a lot of that kind of family interaction in my practice. I’m fine with it. If it’s something within my control, I’ll fix it to the best of my ability but most of the time, the issue is not something within my purview. I listen and sympathize and try to give constructive suggestions. And realize that being there and letting them vent is probably the best thing I can possibly do. But it does get wearing.
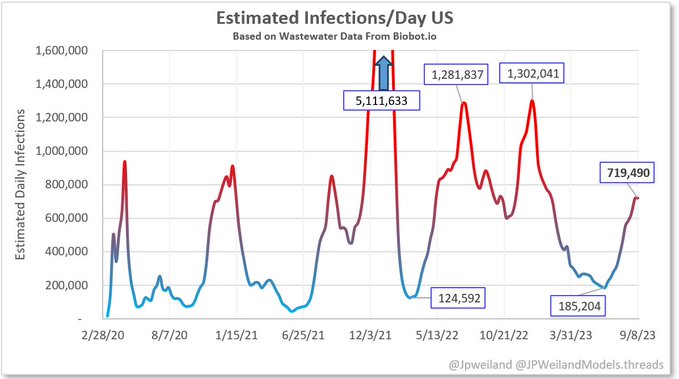
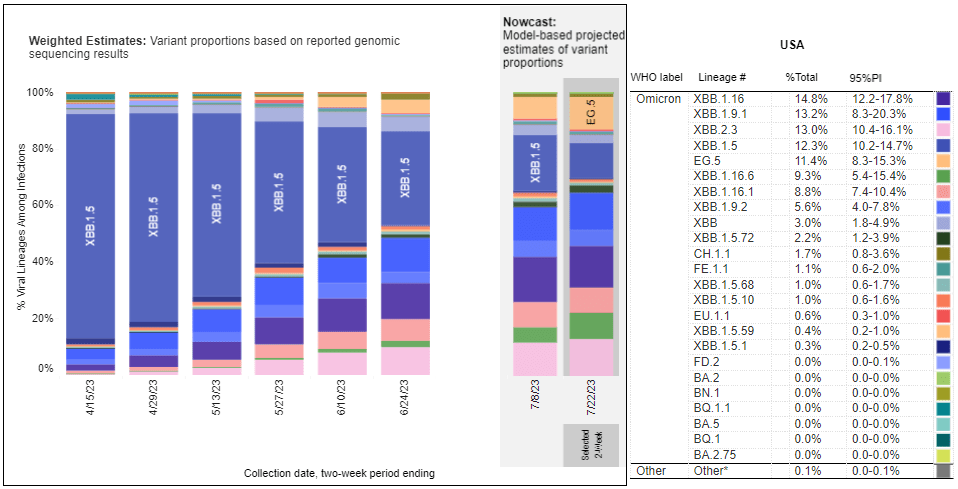
No need to remember when cuz everything old is new again… Here I am going through the page proofs of the third and supposedly final volume of The Accidental Plague Diaries while out in the greater world, Covid numbers are skyrocketing. An article came out in Fortune this weekend in which a number of experts opine, based on wastewater samples and other data, that the current surge is on track to equal or surpass the surge of late 2020 or the Delta surge of 2021. The numbers they quote are of 650,000 new infections daily (with roughly 2% of the population currently acutely infected) and the expectation that up to 30 or 35 million will become infected during this wave before things calm down. These are some scary numbers but there are some differences between then and now.
A majority of the country, despite the loud and media amplified voices of a belligerent minority, are vaccinated and most have had a booster or two in their somewhere. The majority have also caught a case of Covid at some time in the last three and a half years giving their immune systems a good defensive primer on the virus and something to build from should they become reinfected. Therefore, the rate of serious clinical disease is not skyrocketing as it did with previous waves. Yes, hospitalizations are climbing. They were at a nadir around June and they climbed about 20% over the summer and they’ve put on another 5-10% in the first half of September but they are nowhere near the numbers that brought the health system to its knees. However, the health system is nowhere near as robust as it was in 2020 given the protracted effects of the pandemic on finances and clinical staffing so smaller insults may have much greater effects going forward. The death rate is also beginning to climb but I haven’t been able to find really good numbers nor numbers that distinguish between deaths from Covid and deaths with Covid.
I’m not panicking (other than at the thought of having to produce a fourth volume in The Accidental Plague Diaries). I have had it twice and had My original shots and three boosters. I’ll get this newest booster as soon as it’s available. When will that be? I don’t know. We keep hearing ‘October’ so hear I sit under the tree like Vladimir and Estragon waiting… I’m also not certain that I want to stake my life planning on an article that appears in Fortune. It’s not necessarily the most pre-eminent of scientific journals. I would like to see this confirmed in more reputable sources and I would love to see some better real time tracking numbers. Unfortunately, with the end of the public health emergency in May, we more or less disassembled a coherent federal response and turned everything back over to the patchwork of state, county, and city public health agencies where the collection and dissemination of data is now somewhat dependent on local politics.
So what do we need to do? Get the new booster (which has been reformulated to work better against current circulating omicron strains) when it becomes available. Should you mask? That’s a tough one. Masking works best when it is universal as it’s more about protecting others from you than it is you from others and it requires a cultural paradigm of care for ones fellows as much as for oneself. If there’s anything the cultural history of the pandemic era has taught us, it’s that that particular ethos has more or less been tossed out the window for political expediency and there are now laws preventing mask mandates in various places. Masking when the world does not won’t hurt you. It might help some. The other thing to do is get back in the habit of keeping those hands washed and sanitized if you’ve gotten out of it. The litany of 2020 still holds true.
On to other topics. I should have the page proofs fully checked and back to the publisher by the weekend of the 23rd. Allow two weeks for those corrections to be made, another two weeks for proof copies to be printed and checked, and then I can announce a publication date for Volume III. Should be just before Halloween. Incidentally, the cover is orange and black which I suppose is fitting. We decided to go with secondary colors for the series. Green/Purple/Orange. Don’t make me have to go all primary as well. The chapter titles come from the work of my third favorite Broadway lyricist after Sondheim and Cole Porter. You’ll have to read the book to discover who it is.
My theater/music calendar is shaping up for the 2023-2024 season. I’m thinking I need to create a graphic like my professional opera singer friends with all my gigs listed out. Unfortunately, a few things are still in flux so I can’t do that as of yet. It looks like a symphony concert (and maybe two) and a play prior to the New Year and a couple of stage appearances, another symphony concert, and a directing gig in the first half of 2024. Should keep me out of trouble. More details to come as things like contracts are finalized.
I went and saw Virginia Samford Theatre’s production of the Rodgers and Hammerstein revue, A Grand Night for Singing, last night. Four of the five performers were old friends whom I have known and worked with for years. The fifth has relatively recently come to town and I hope I get a chance to share a stage with him sometime. R and H is not everyone’s cup of tea these days but boy did they know how to craft a song with a melody and a relatable lyric. The five performers are all terrific in their own right but what blew me away was the blend of their voices when they sang both unison and harmony arrangements. It really did sound like a single unified vocal. Kudos to Debbie Mielke for her work at the piano and with the performers to achieve that. I went to the show with a few friends from church. We met first for dinner at a local Indian restaurant which recently had to relocate after decades. Taj India, now in the late lamented Bogue’s space, remains as good as you remember. Nothing has changed in the kitchen. Ten minutes before we left to go to the theater, the skies clouded over and the sunny day turned into one of those Southern gullywasher rainstorms that drops several inches in the course of half an hour. Intersections were flooded all over the Southside and visibility was near zero but we managed to get to the theater on time, albeit much wetter than we had intended.
I need to start thinking about putting my life together for my trip to Eastern Europe in a couple of weeks, lord willing and the Covid don’t rise. But that’s just modern life. You make your plans and you play the hand that nature deals you, whether it involve infectious disease or planetary change from climate or other issues. If the travel posts start in early October, you’ll know I’ve made it. In the meantime, there are clinics to conduct, house calls to do, legal cases to review, a book to finish, and various choral rehearsals. Plus the occasional Dungeons and Dragons game. We’ve discovered the joys of playing over brunch with mimosas. Highly recommended if you game as an adult. Bandon the cleric has to arm up later this morning for continued adventures in the Feywild.
He washes his hands and believes in the magic of vaccines.
I’m having a lazy Saturday. I don’t get a lot of those. Usually I have to dedicate it to production issues on a show or play major catch up with work but the combination of being between theatrical engagements coupled with the short work week due to Labor Day has led me to a day where I don’t have to plan my time around a whole series of ‘must accomplish’ tasks. There are a few on the list, but none of them has to be done before next week and I have little happening tomorrow besides church and a callback in the evening so those can be safely put off until tomorrow afternoon. The weather has calmed down from infernal to relatively pleasant midsummer so I may take myself out for a walk a bit later.
I like walking. It’s one of the reasons I enjoy traveling to Europe so much. European cities, at least the historic centers where one spends time as a tourist, were all developed when the chief mode of transportation was by foot (or the occasional horse and ox cart for heavier goods). The areas are compact, not devoted to the automobile and parking, and there’s always something interesting to look at in the shop windows. My pedometer shoots up when I’m on vacation from my usual 4-7,000 steps a day to something in the 15-25,000 step range. It’s a healthier way of living. You can see it in this country in people who live in those few urban centers developed prior to the 20th century and the automobile where the general population relies on public transportation and their own two feet. I read somewhere that life expectancy in Manhattan is several years longer than it is in the outer boroughs of New York. The difference being that Manhattanites tend to walk and those in the more suburban areas take their cars.
I leave on my next trip four weeks from yesterday. I’m getting all my ducks in a row regarding the paperwork, proof of Covid vaccination (no, I still don’t know when the next booster is going to be available – the last I heard was October sometime), making sure I have what I’m going to need in terms of travel supplies and putting my compression socks through the wash. I discovered several years ago that this latter was necessary for me on international flights, otherwise I get off the plane with 3+ pitting edema. My first stop is Krakow and then it’s down to Bratislava and up the Danube through Vienna before eventually ending up in Berlin. I looked at the itinerary and saw that the hotel I’m staying at in Berlin is the Adlon. That earned a major ‘Squee’ from me (and would from anyone who has been involved in as many productions of Cabaret as I have been.)
The major project of the next three weeks is to do the edits on the page proofs of Volume III and Volume the last of The Accident Plague Diaries so we can get it out this fall. It’s been a bit delayed due to life issues with my editor but there’s no huge hurry. In some ways, I’ll be glad to be done with the project and in others I’m wondering and worrying what will arise to fill that life gap. I’ll continue to write these pieces but now that I actually will have roughly 1,000 pages and 300,000 words out there in multiple award winning books, I feel a certain obligation to myself to come up with some new writing project that will build upon earlier success. I think I owe it to myself. But I’m not going to make any decisions nor begin anything until all three volumes of The Accidental Plague Diaries are out there. If any of you have an organization that wants to sponsor a reading or a connection with a bookstore that would like me to do a reading/signing, let me know.
So where are we with Covid? It’s causing a significant impact in the local hospitals at the moment, not because the wards are filling up with people dying of lung complications. Admissions, while definitely up over what they were earlier in the summer, are still way below previous surge numbers. The issue is that it’s becoming so widespread that a significant percentage of staff are out on quarantine on any particular day making it difficult to provide adequate nursing and other ancillary services. The physicians aren’t exempt. It’s been running through the residents like crazy the last few weeks. I haven’t gotten it this time around – at least to my knowledge. I suppose it’s possible I’ve had a subclinical case without enough issues to cause me to pause and test myself. Both times I’ve had it, I’ve known I’ve had it with severe symptoms for a day or two and I have had nothing like that although I have had an occasional drippy nose or irritated GI tract.
Looking through my usual Covid news sources, the news is mixed. On the down side, numbers are definitely up nationally and waste water surveillance and other public health measures show a rise of new variants, especially BA.2.86. On the up side, morbidity and mortality numbers, while up from their nadir, are not surging forward as they have in the past suggesting that the combination of vaccines and native infections with antibodies are holding the line. The new variants all remain omicron sub-lineages. There hasn’t been a radical mutation away from that yet. Preliminary data shows that the new vaccine formulations for the booster will be effective against them and that Paxlovid therapy is still working. Big sigh of relief. I don’t believe for a minute that there won’t be some sort of significant new strain coming down the pike in the next year or so and I hope it’s not something with a particularly nasty surprise up its sleeve.
Next task is to call my sister and tell her to get the cover art for Volume III to my editor/publisher. It’s the same character, but in a very different mien, looking a bit how I feel when I contemplate the state of Geriatrics both locally and nationally. I had my annual review yesterday. You will all be happy to know I will continue to be employed next year. My checking account will be happy.
And we’re on to another month, the ninth of this year. In some ways, the year has flown by and in others, it has dragged on at a glacial pace. I no longer trust my perception of time. It’s another gift of the pandemic. That enormous interruption in the usual routines of life and the Groundhog Day repetition of the shut down threw everything all catawampus in regards to my usual understanding of the measured order of time and season and I find myself confusing things that happened six months ago with those that happened six years ago. And things that happened pre-Covid in some ways seems clearer and nearer in time than things that happened in the last year or so. We’re only four months away from the pandemic’s fourth birthday (the first reports of what we would come to know as Covid having been filed in Wuhan on December 31, 2019.) I prefer to think that these wrinkles in personal time are due to psychological coping mechanisms that come into play in times of great societal stress and not the first symptoms of incipient dementia. I feel my mother’s hereditary variant of Pick’s disease hanging over my head from time to time. Fortunately, it doesn’t strike until after age 75.
12 Angry Jurors closed last night. It ended up being quite a good show and was both an artistic success and a success for the company as it encouraged people in Birmingham interested in live theater who had never been to the venue to come check it out. The Encore Theater is the only African-American theater company in town with its own stage. I got to know Marc Raby, the founder and artistic director just after it got up and running when we were cast opposite each other in a production of Choir Boy. We decided we quite liked each other and I’ve tried to help Encore in my own small way at various stages in its development. By doing a larger cast play with a multiethnic cast, they stepped outside their usual wheelhouse of African-American entertainment for African-American audiences and showed that they could put up as engrossing a production as any theater in town. The production was inexpensive, but it was so well cast and the cast truly performed as an ensemble (all the other cast members besides me were onstage for the entire two hours of the running time. I wandered in and out a few times, mainly as a plot device) that the end result was a powerful piece of theater and audiences ate it up.
That’s the end of my scheduled theater life for now. I have a performance of the Faure Requiem with the symphony chorus in October and a show I was cast in last year and which was delayed until this year is scheduled for December. But I am not sure if I will continue with it. It really needs to go into rehearsal early October and I am out of the country from the 6th to the 22nd. I have submitted self tape auditions for a couple of things – a comic monologue for The Man Who Came to Dinner (I have a callback next weekend) and a song for Into the Woods. (No word on callbacks for that one yet – but the Narrator/Mysterious Man part has my name written all over it). My choice for audition song was Kurt Weill’s September Song from Knickerbocker Holiday as Weill is about as close as you can get to Sondheim without singing Sondheim. As I listened to the tape before submitting, I was rather surprised with how decent I sounded. The voice lessons are paying off.
Let me just say that I hate auditioning. I always have. At least the pandemic has rewritten the rules somewhat and we’re not doing as much cattle call sit around the lobby. Rush up on stage, sing your song with an accompanist you don’t know and then try desperately not to fall over in the dance call where you’re feeling like that guy in the ‘On Broadway’ sequence from All That Jazz and wondering why you’re up there as you wrote all over the audition sheet that you aren’t a dancer and never have been. Most of my on stage dancing in recent years has been box step waltz in operetta and that I can handle. I can still do the Hustle as well but there isn’t much call for that these days. Maybe if I get cast in Xanadu. Now we set up an iPad and film ourselves as we emote or sing and send the file off to the theater company where they probably get infinite joy nitpicking on the mistakes. September Song is a good fit for my age and type. I just wish the published key was about a step lower. I can sing it in the published key (and that’s what I submitted) but it would sit better in my voice just a bit lower.
I was looking earlier this week at a study out of UCSF wherein the researchers estimated that in the coming few decades, roughly 25% of the population that will develop dementia will be living alone without spouse, children, or other informal in home supports. For this geriatrician, that’s a rather frightening statistic because I see all of the things that happen when an older adult ages into dementia without an appropriate support system. Finances go to hell as the individual doesn’t understand the basics of math and the moving of money. Bills aren’t paid (or are paid multiple times). Junk mail that looks like bills are treated as such and soon checks for thousands of dollars are happily sailing off to scammers in Jamaica. Taxes are forgotten. Cars are repossessed. Properties are sold at auction without the occupant understanding what’s going on. Driving is a relatively automatic process and demented people tend to operate cars fine. However, navigation is not and the trip to the grocery store ends up with them running out of gas in a neighboring state as they missed the exit, didn’t realize it and just kept on going as they kept looking for it. Getting food on the table is a very complicated process in our society which involves getting out to the grocery (usually farther away than walking distance), navigating the store, affording the bill, schlepping it all home, storing it properly, and then preparing it in the right way at the right time. Things go wrong all along this food chain which is why often the first physical sign of dementia is weight loss. And don’t get me started on trying to manage medications and health appointments when your brain doesn’t work properly. I’ve said for years that in geriatrics we don’t have appointment times, we have appointment suggestions as cognitive issues keep many of our patients showing up at the wrong hour, the wrong day, even the wrong year. Geriatricians know that no adult human being will take medication more than twice a day with any sort of regularity (morning and evening). We work like hell to get medical regimens down to that and then our colleagues in various subspecialties show up and put them on something three times a day, something four times a day, something before meals, something that can’t be taken within two hours of food, and something that has to be half an hour before other medications. Forget it bub… it ain’t happening.
I’m fast forwarding in my head twenty years to 2043. The lead edge of the Baby Boom, the 1946 babies, will be turning 97. (Cher, a 1946 baby, will be on yet another farewell tour). The prevalence of dementia at age 90 is about 60% and at age 95 is about 80%. Most of the early boom will have cognitive impairment and we have done nothing as a society to prepare for this eventuality, regarding it as a private matter rather than one for public solutions. But, as this study says, about a quarter have no private social capital on which to rely so we’re either going to have to have some sort of public system for them or we’re going to have a whole lot of nonagenarian bag ladies all over the boulevards. But that may be the plan, at least on one side of the political aisle. Don’t fund elder services and hope they die fast. I have news… people, if given the chance, will live a great deal longer than you think they should.
It’s nearly 8 PM on a Sunday. I am finally finished with the 37 progress notes I had to write this weekend and my eyes are a little bleary. But that may be the peppers in the left over Szechuan chicken I had for dinner still tap dancing across my nasal and lacrimal tissues. I’m all for capsaicin in my food but a day or two in the refrigerator seems to have leached out a bit more than usual into the fried rice. I really don’t like devoting hours every weekend to finishing up progress notes but it’s one of the curses of primary care medicine. I could do them as I go, but to do that I’d have to cut about ten to fifteen minutes of face time off of every visit and that extended face time is what allows me to be a healer, so that’s not really an option. I could do them in the evening but it’s usually the last thing I want to do after a long day, especially if I’ve had to go from work to rehearsal and am not getting home until between 9 and 10 pm. That leaves the weekend. I tell my patients frequently that on the day I retire, I am going to take one of the EHR computers over to the atrium and drop kick it off the third floor landing. And I’m only partly in jest.
UAB is full and the ER is swamped this past week. I haven’t been able to get a good read on how much is related to Covid and how much is other things. I’m guessing some of it is heat stress on aging and otherwise unhealthy physiologies. We continue to be mired in the high 90s low 100s with high humidity around here making outdoor activity uncomfortable at best and downright dangerous at worse. I don’t go out in this weather. I stay in air conditioned office, air conditioned car (fully recovered from this last week’s little adventure), and air conditioned condo. The complex pool is right next door but it’s too hot for me to even want to walk over there. Covid hospitalizations and deaths are both up about 20% over last week per CDC data and have been steadily increasing all summer. We’re not back where we were by a long shot but all the trends are heading the wrong direction.
Another week, another mass shooting, this one at a discount store in Jacksonville, Florida. By all accounts it was perpetrated by a radicalized young man full of racist and misogynist hate as an act of violence against African Americans. Ron DeSantis turned up at the public memorial today and was promptly booed and had the mic taken away by the assembled crowd. Who could imagine that his policies of allowing anyone to purchase semi-automatic weapons and demonizing minorities would lead to actual tangible results? The stochastic terrorism coming out of the right wing is going to continue until such time as the population as a whole rises up and states enough. I’m not sure when that is going to happen. The politically active classes in our society are far too comfortable in their gated communities, insulated from real concerns by various structures of privilege to flex their muscles as of yet. Someday they will wake up to the fact that they traded the lives of their children and grandchildren for slightly better returns on their 401Ks but today is not that day.
My background in rural health and home care/house calls means that I have been in all sorts of homes over the decades. Apartments inhabited by extended families of newly arrived immigrants, trailer homes of the impoverished rural with the meth lab out back, waterfront palaces, old money mansions smelling of slightly decaying furniture, tarpaper shacks with more animal residents than human. They were all home to someone and home, whatever it may be, exerts a powerful force. I have learned over the years to not stick my nose in things that are not my concern (like the odd person that crawls out of the pile of dirty clothes in the corner and lurches naked to the bathroom), to honor that the place in which I am a guest usually represents a culmination of living and life choices, and to enter into a healing partnership with a patient and family, not march in and lay down the law like some white coated Moses bearing the tablet in the form of a prescription pad.
In times past, at least in cities, the rich and the poor lived cheek by jowl and had at least a limited understanding of each others lives. The invention of the automobile and then the suburb changed that balance and the rich tended to withdraw into bubbles that the poor could not penetrate and left the poor to separate cultural and geographic spaces. Occasionally, due to geography or other factors, they are thrown together again. San Francisco, now being held up by the right as a failed city, is one such place. It isn’t failed. It’s just a city where the rich and poor exist in tight geographic proximity and the rich are forced to confront the real lives of the poor and what fifty years of vulture capitalism has actually accomplished.
I often take med students and residents out on house calls with me. Usually I have one or two a year who is a native Birminghamian, almost always from one of the neighborhoods known here collectively as Over The Mountain (translation – wealthy and white). I take them to places within twenty miles of where they have spent their lives and into homes that they have no idea exist, having never been invited into the home of someone who is not of similar caste. I’ve never lived Over The Mountain. I’ve lived on it but always on the city side. And I don’t feel uncomfortable in neighborhoods and homes different from my own. I figure it’s my time to learn about different ways of living and different perspectives on all sorts of things.
The show I’m currently rehearsing, 12 Angry Jurors (12 Angry Men for a mixed gender cast), is being produced by the only African American theater company in town with its own stage. They usually do African-American shows for an African-American audience but they’re reaching out with this one with a mixed race cast trying to reach a wider audience. Usually when I attend their shows, I’m one of the few white faces in the audience but I am always made welcome and most of the regulars now know me. I would like to challenge my Birmingham theater friends to come on out to this production, explore a new venue, help support artistic excellence for a different group than you usually support. You might be pleasantly surprised.
It’s been a Monday on a Wednesday. Or something like that. Actually, it’s been Monday after Monday so far this week as things are piling up rapidly. Fortunately, I have a slow weekend so I should be able to begin getting things caught up. The Mondays began with the second weekend of performances of A Midsummer Night’s Dream. It ended up being an enjoyable romp in the woods for both cast and audience and there is already talk of another Shakespeare for next summer. I’m not against it. Of course, the one I would really want to direct is King Lear as it’s one of the only works of Western Literature to deal with the catastrophic effects of dementia on family systems – but I don’t think this group is quite ready to go there yet and we better stick with Much Ado About Nothing or Twelfth Night or maybe The Tempest.
And then it’s been multiple issues of craziness at work. The chief one being the flooding of the building in which my VA office is located (burst water pipe). The damage appears to be relatively extensive and despite the multiple Servpro trucks parked all around the block, we’ve been told we cannot get back in for several months. I’ve had to transfer my VA office to my home office for the duration which took several days of cursing various computer systems until I could finally work with the charting system and get into my email. On the UAB front, it appears that all of my patients have decided that this is the week to write long emails through the portal system with multiple clinical questions – and we’re running short staffed due to vacations and illnesses.
To top it all off, while driving on the interstate late this afternoon, through the aptly named malfunction junction (where I-20, I-59 and I-65 all converge just west of downtown), I had a blowout in my right rear tire. Fortunately, I did not lose control of the car, was able to get off the freeway and into a gas station parking lot, and then spent the next several hours in a low budget version of Planes, Trains and Automobiles while I attended meetings on Zoom while dealing with AAA, the Toyota Dealership, a ride across town in a tow truck with a most amiable driver, and a trip in an Uber with a guy who did not seem to understand the function of traffic lights. Needless to say, I am now at home and contemplating a large single malt scotch before bed, something I rarely do these days but I think I deserve it.
So where are we with Covid? It’s definitely everywhere. I’ve been informed that someone who was at the wedding I was at this past weekend has been diagnosed. One of my Midsummer actors tested positive this morning. There was a case in the cast of Twelve Angry Jurors last week. I’ve had a couple of messages a day from patients who have tested positive. The local ERs are full. Hospital rates are still relatively low but anything could happen. Most of what is still circulating are omicron variants. They’ve been given various poetic nicknames such as Eris and Pirola but they are pretty much slightly mutated sub lineages of the omicron that raced through the world during the holidays of 2021. There are some new variants percolating though which, while not widespread yet, could create problems moving forward, especially BA.2.86 which has dozens of variations on the spike protein (important because that’s how the virus latches on to host cells). It’s very different from omicron (although I haven’t seen it assigned it’s own Greek letter yet) and worldwide surveillance has detected it in several countries. Wastewater surveillance has found it in even more places suggesting that it’s spreading undetected through the community. Will it cause a new spike in cases or morbidity and mortality? Time will tell.
People keep asking me what do we do? As politically, we are not going to go back to lockdowns or mandatory masking unless there’s a strain that causes a severe increase in mortality and morbidity in young healthy people, the options are relatively straightforward. You can masks, but unless masking is universal, it’s not all that helpful. If you have been diagnosed, you should mask to protect others for ten days (five days on isolation, five with masking but you can go out). If you have had a known close exposure (fifteen or more minutes within six feet of a known case), you should mask and test if you have symptoms and if asymptomatic, on day five. If you’re negative, the mask can come off then. Probably as important as masking is keeping your hands washed. Thank god my new UAB office suite has sinks in the patient exam rooms (we didn’t have those in our old suite). My hand hygiene is pretty good as I wash before touching a patient. Isolating yourself is an option, but I’ve got too much going on in life so I choose not to at this point. I’m fully vaccinated and boosted. The next booster (which should continue to help against omicron strains. I don’t know about BA.2.86) is supposed to be released sometime this fall and I will certainly get one. I have no more information on when it might be available than anyone else.
I had my first church choir rehearsal of the season this evening, start up with the Alabama Symphony Chorus in a couple of weeks (first up is the Faure Requiem), have been making progress in my voice lessons and have a taped audition for ‘Into The Woods’ due next week so lots of vocalizing around the condo at the moment. The cats are trying to sing counterpoint but they always seem to come in in the wrong key. I’m pretty happy with my audition piece and I hope it’s enough to land me the Tom Aldredge double casting. That’s my role. Although it’s a show I love dearly and I’ll settle for whatever.
Thirty some progress notes, a new legal case, and a lecture to write all teed up for this weekend. Thank god the bailiff in 12 Angry Jurors only has four lines. I was off book walking across the parking lot to my first rehearsal. We tech and perform that next week. Then I think I’m off from things theatrical for a couple of months. It’s probably just as well.
We’re half way through the second weekend of A Midsummer Night’s Dream and the show is holding up well, getting tighter and tighter as the cast becomes more comfortable with the language and more willing to take the play up to comic brio tempo. I’ve managed to arrange things to be at every performance so far, but I’ll miss tomorrow’s as I have a wedding to go to and I promised to attend nearly a year ago. I’ve known one of the brides since she was a child and have enjoyed watching her grow and mature into an accomplished young woman. I will catch the closing performance of Midsummer on Sunday… and be back in rehearsal for Twelve Angry Jurors on Monday. Fortunately, in the latter, I’m playing the bailiff and have all of five minutes of stage time and four lines so it’s not a huge strain.
Covid numbers are continuing to increase at a somewhat alarming rate. Hospital numbers are increasing at about 10% a week (which means doubling every month and a half) and new variants are popping up. They all appear to be omicron strains so far but I won’t be surprised if we move on to a new Greek letter before the end of the year after some radical new mutation comes to light. I don’t think we’re going to go back to the kind of numbers we saw in 2020 and 2021 as vaccines and natural immunity are now widespread but anything is possible and the general weakening of the health system and public health mechanisms in general are going to put us in a bad position if something major comes down the pike. The ER at UAB and the VA has been filling up again but I haven’t been able to track down how much of that is due to Covid and how much is due to other causes. Our unrelenting heat wave is certainly making people with chronic disease more prone to an exacerbation due to dehydration and heat exhaustion. Still haven’t heard any specific information on the availability of a new Covid booster this fall. We’ve been told it’s coming, but not when or by what means. And it’s likely to cost you. The expiration of the emergency back in May means that the federal government is no longer picking up the vaccine tab.
We’ve been lucky with Midsummer that Covid has stayed out of the cast. (Knocking every piece of wood within reach of my arms). Other local shows have not been so fortunate, having to cut runs short or to rapidly redo rehearsal schedules after a couple of people have gotten sick. And it’s happening elsewhere as well. Josh Groban is out of Sweeney Todd on Broadway due to Covid infection. I’m sure his understudy is perfectly competent but people are paying hundreds of dollars a seat for the star. Cancelling shows, which is extremely disappointing to the cast and crew whom have worked so hard, is also financially devastating to small companies that depend more on box office than the larger rep theaters which get much of their operating budget from grants and major donors. The finances of the American theater industry are in a complete turmoil currently and a lack of performance certainty isn’t helping anyone at any level.
Should we go back to masking? It might not be a bad idea but it only truly works if everyone does it. You don’t so much mask to protect yourself but to protect others from you. If everyone masks, transmission declines. If only a small percentage do, it doesn’t make much difference. You can protect yourself with masking, but really only with properly fitted N-95s which are devilishly uncomfortable to wear. There’s certainly no political will to go back to mandatory masking in this part of the country and even locales with a better track record are going to have a hard time with requirements without a major shift in public opinion (which will probably rely on a major shift in mortality and morbidity statistics).
Speaking of mortality… As they continue to dig more bodies out of the ashes of Lahaina, I’m looking for information as to who the dead are. I’m expecting that we’ll find that most of them were members of what I call the invisible population. I see them because of the nature of my work but most of us never meet them because they rarely appear in public space. They include older individuals who have become physically weaker making it difficult for them to navigate public space without a wheelchair, walker, and the assistance of another person or who are losing mentally capacity and who rarely leave the familiarity of home as the complexity of the outside world is too much for them to handle. They are the morbidly obese who have difficulty leaving the house. The bed and chair bound. The seriously ill who have feeding tubes and catheters and oxygen at home. The relatives who may be able bodied but who are devoted to caring for an incapacitated person and who would not dream of leaving them behind in an emergency. They could not possibly outrun a fast moving firestorm with limited warning. We don’t think of the invisible population because it’s convenient for us not to. Their lives are usually governed by laws and bureaucracy put in place by well meaning people with no practical experience in the issues that the invisible face.
I’ve spent my professional life with the invisible. One of the reasons I’m as effective in my job as I am is that they understand that I am one of the rare authority figures in their lives that truly sees them when most do not. I enter their houses. I hear their hopes and fears and dreams and do my best to at least help them achieve what little balance in life their bodies will allow. But, because I work with the invisible, I and my medical specialty are rendered invisible to the majority of the American health care industry. We in geriatrics don’t generate money or brilliant cures or major headlines and this makes us an afterthought at best or, as one of my internal medicine colleagues once told me, ‘Geriatrics is just Internal Medicine when it doesn’t matter’. Geriatrics as an official boarded specialty isn’t that old. It began the same year that I graduated from medical school so I am the first generation that was formally trained in the subject. And I have watched my entire career as it has been shunted aside and is now in a state of collapse, with the looming retirement of the initial cohort of geriatricians, just as the demographics of the country require the knowledge base with the aging of the baby boom. Jerry Gurwitz, the head of Geriatrics at the University of Massachusetts wrote an Op-Ed in the Journal of the American Medical Association thoroughly discussing this issue which is worth reading. You can find it if you google. (Or at this link https://jamanetwork.com/journals/jama/fullarticle/2808221)
How do we make the invisible visible? Danged if I know. But I have an idea of where to start. We’ve changed the culture away from one which idealizes progress and community to one which worships only material gain. I don’t think fundamental change is possible until we start turning back the other way. That used to the role of religion but that seems to have failed as badly in America as our politics and our economics. This is all making my head hurt so I think it’s time to end this post and put on bad TV. After all, tomorrow is another day.
I’m tired of writing about Covid. I really am. A thousand pages and three hundred thousand words of The Accidental Plague Diaries was enough to exhaust me on the subject and everything I could possible say about it. But, as much as I may be done with Covid in this the first ‘normal’ summer since the summer of 2019, it is not done with us. There’s been very little media coverage of current pandemic trends but medical social media has been starting to light up over the last few weeks with all sorts of ominous warning signs. The prevalence of virus in wastewater samples doubled over the course of July and is still increasing rapidly. Pediatric admissions in the greater New York area are at their highest since the summer of 2020, the early days of the pandemic. Lab test positivity rates are soaring in various spots. It’s difficult to get confirmation on these reports or truly see national trends. The CDC website seems to be the best source for up to date information currently but it’s only as accurate as the data being forwarded to it by our patchwork system of public health departments, many of which are not functioning well in the wake of pandemic burnout and political chicanery.
The local numbers here in Birmingham seem to be increasing, but not soaring and, from what I can tell, hospital numbers and death rates haven’t increased appreciably but those are lagging indicators and it may some weeks before they start to rise in response to the current increase in infection rates. As our long hot summer continues (and I cannot begin to tell you how tired this Seattle boy is of temperatures in the 90s with high humidity), there is a continued push toward indoors with air conditioning activities and, given climate change, we may be looking at continued summer waves of infectious disease due to this phenomenon. What am I doing personally? Living my life. Planning on a fall booster. Keeping my hands washed. I haven’t gone back to masking in public yet but that may be coming.
A Midsummer Night’s Dream, which seems to have suffered from every other disaster imaginable during its rehearsal period other than a Covid outbreak amongst cast and crew, opened last night and I couldn’t be prouder of the company for the end result. Sixteen performers, many of whom had never worked with Shakespearean text and a crew of seven came together and, with a budget approximately equal to what would spend at McDonald’s to feed a family of five, created a fast moving, funny, summertime romp through the woods which engrossed the audience and kept them chuckling for two and a quarter hours. As for my work, I don’t know how to gauge it. I can never judge my own artistry as a performer or creator. The one thing I can judge is that I think I met my goal, which should be one of the chief goals of any community theater, and helped build an ensemble, a community out of disparate individuals, getting them to create something that none could do on their own. Each actor or technician brings something unique to the show and I have favorite moments from all of them. (Including a last minute gag thrown in final dress involving a white plastic chair – it’s very Alabama).
I’ll turn up at all the performances I can to cheer them on from the back but my job is finished. I’m not sure what’s next for the theater career. There’s a couple of things out there in the ether and I have a few auditions I have to put together this next week. Once things are settled and contracts are signed, I’ll let people know. I’m pretty sure that whatever it is will not involve directing Shakespeare. I wouldn’t mind doing it again but it does take a lot of thought and mental energy to turn those four hundred year old texts into something fresh and relevant to today. They are so brilliantly written that it’s possible and will always be possible. Except, perhaps in the state of Florida where school districts are banning high schoolers from reading the plays due to ‘racy’ elements and replacing them with ‘excerpts’. Really. They should just shovel the whole canon into the dumpster and replace them with copies of Lamb’s ‘Tales from Shakespeare’ and go full early Victorian. The bowdlerization has already been done. Don’t waste effort.
I’m just getting to the point where I’m rolling my eyes at the political news from all over. The sense of desperation in word and action rolling off of the Republican party as it crashes into the unyielding walls of demographics, science, and cultural attitudes would be funny if it didn’t have such real world consequences. They hitched their wagon to a particular star and I think they’re about to find out that actions have consequences. We may find that eventually the GOP is going to go the way of the Whigs to be replaced by another conservative party that will accept logic, science and reality. But I’m not holding my breath.
I’m very sad about the news out of Maui regarding Lahaina, a lovely town which I have visited many times and was a particular favorite of mine and Steve’s. We made a number of Hawaii trips together during our years in California as it was our tropical beach getaway. Steve hated seafood (he always ordered Chicken when we went out to dinner there) but he loved the ambiance of sitting on the terrace at Kimo’s with the waves lapping just below our table. We were having dinner there one night, sometime back in the 90s when a large bustling family group came in and proceeded to get rip roaring drunk at a nearby table. Everyone, that is, except the babe in arms (although I really don’t know what was in his bottle). Late in their meal, grandpa got up and picked up the baby and was dancing around the room with it when he tripped, fell and the baby shot out of his arms and struck a planter. The baby, being none to happy about this, began to wail, the mother began to shriek and, in her desperation to reach the baby tripped over grandpa and down she went. She got up with a bloody nose. The sight of the blood made someone at another table vomit their dinner all over the place. We decided it was a good time to leave and made a beeline for the lobby and paid our check there. We had no interest in remaining in a scene straight out of the Marx Brothers.
Time for me to head off to today’s performance of Midsummer to egg the cast on to another great performance.
I came home from work today around 4:30. Laid down on the bed intending to take the weight off my feet for a few minutes and woke up several hours later. I guess it’s the end of another work week full of the usual craziness of aging adults and their families, to be made even more fun this week as it’s my weekend on call. Things dealt with over the last few work days include a sixty something alcoholic in a shot house full of drifters who can no longer walk, a demented older woman who decided the best way to greet her sitters was with a hammer, a family who are demanding that we find some way to care for their bed bound dying relative other than through hospice services, and a chronic pain patient with whom I had the same lengthy conversation I have every six months or so on why increasing opioids to narcotizing levels is a really bad idea when you’re in your late eighties. It never ends. In some ways it feels like it’s gathering steam and rushing at us faster and faster. I don’t know if that’s the changes in mental and physical health courtesy of the pandemic or if my rather deep well of patience is finally starting to run dry. We shall see.
Speaking of the pandemic. Here’s the latest. It’s not easy to find good data these days what with the end of the emergency and the dissolution of central public health data collection back to the patchwork of fifty states 3,000 counties and 350 cities that make up the country. From what I have been able to piece together, the number of Covid cases has roughly doubled over the last month and seems to be on the increase. The most reliable testing these days is wastewater surveillance which can be done passively on populations and it seems to bear this out. Rates seem to be a bit higher in the southern US than the northern, likely due to the hot weather and people indoors in poorly ventilated public spaces trying to escape from the excessive heat. The good news is that even though the number of cases seems to be increasing substantially (and I hear of a friend testing positive pretty much on a daily basis), the number of hospitalizations for Covid and Covid complications hasn’t gone up significantly. The wall of immunizations and natural immunity from prior infection seems to be holding for now. Will it continue to hold? Who knows. I keep getting asked if another booster is warranted. The latest is that a fall booster is reasonable for those in older age groups or with immunocompromise. Not because there are nasty new variants making the rounds, but because the effectiveness of the vaccine seems to wane some with time and giving it a boost seems to help with overall protection. I’m currently planning on getting a boost in September for myself but I am watching various medical news sites to see if there’s better or updated information before I make a final decision.
One week, will it never be right? This time next week A Midsummer Night’s Dream will be up in front of its first paying audience. It’s coming together and there are some very good things starting to happen on stage and most of the cast are bringing their full energies to the proceedings. There are a few who need to spend the next few days with their noses buried in their books and a few others who need to get a little less distracted in rehearsal by non-show related things but that’s typical. I can see the show I want an audience to see coming to life within all of the extraneous issues we’ve had to deal with (injuries and illnesses, tech issues, missing pieces) and ultimately it’s going to be comic romp that it needs to be and which I think is close to Shakespeare’s original intent. He didn’t write it as a high falutin comedy of manners for the court, he wrote it as jolly good time for the groundlings. Next week will be the last few chances to bake the souffle and hope that it doesn’t fall flat when it gets pulled out of the oven.
Blue Little Guy Characters Vector art illustration.Copy Space.
Blue man from TV screen shouting with megaphone.
I’m trying not to read too much into the political news of the moment. It’s become clear that a portion of the population has decided to reject science, rational thought, critical reasoning, and basic morality for some sort of primitive tribalism whose tenets and creed depend on the whims of a very small number of people with very high public profiles. They can continue to take over the various political apparatuses that make the country function but, when in the locales they do succeed in imposing their worst instincts, they start driving the educated and rational away, I wonder who they think are going to provide their medical services, run their power grids, keep their banking system operational and all of those other things that depend on science and reason. Faith can only take you so far. The exodus has begun from the universities and medical systems and other highly skilled employment disciplines of Florida and Texas. I wonder who they think they’re going to find to replace them? Given other actions, immigrants are out…
I’ve been asked to appear in a play late this month. I would usually say yest without hesitation but this one opens only two weeks after Midsummer and I don’t think I have enough time to learn the role what with everything going on at work. My sixty plus year old brain just doesn’t learn and retain lines as easily as it once did. I’ll have to take a look at it. If the line count isn’t too heavy and the blocking is relatively simple I just might manage it. Another one of those we shall sees. There seem to be a lot of those this evening.
I feel somnolence coming on again. I think it’s time for a handful of peanut M&Ms and some bad television. If I let myself sleep in tomorrow morning I may be back up to fighting strength. God knows when I’ll get the 19 progress notes unfinished from this week done but that’s an issue for another day.
Facebook reminded me that six years ago today, I was in the pulpit at church and gave the following sermon. Following the wrenching changes of the pandemic, I thought it might be a good time to repost it as it’s even more pertinent now. The political situation is a bit different than it was when this was written but the general underlying issues haven’t changed. If anything, the pandemic has worsened them.
HERE BEGINNETH THE SERMON
Many long years ago, when I was in college, I took a course in modern philosophy. It was full of rather incomprehensible readings by authors such as Buckminster Fuller and Noam Chomsky, most of which I forgot soon after the final. The one piece that has always stuck with me was a unit on what is known as moral reasoning. In it, we were posed with questions regarding what was right or wrong in various scenarios. Our answers were supposed to show how developed we were but probably proved that we were thinking as college sophomores, with all that entails.
One scenario we were presented with was something like this. You are a parent with an only child. Not a situation most of us could easily identify with being in our late teens and early twenties and Stanford students who weren’t thinking about reproducing yet. Heck, we weren’t even thinking about sex all that much. School was pretty overwhelming. Anyway, back to being a parent with an only child. One day, we were told, our child becomes ill with a dread disease. It’s OK though; there is a medicine that can cure them. Off we go to the druggist to obtain this miracle medicine. The druggist tells us that he indeed has the medicine we seek. He created it himself, patented it and is the sole source -no other druggist is allowed to sell it. In casual conversation, he mentions that it costs him about two hundred dollars to produce a course that will cure an afflicted child. However, because he is a good capitalist and has his own expenses, he sells it for two thousand dollars for a course of treatment. We now find ourselves in a quandary. We can only raise a thousand dollars to save the life of our child. No amount of pleading will make him lower his price. We are not about to let our child die so that night, under cover of darkness, we break into the druggist’s shop and steal the medication we need to save our child. The question we were asked at the end of the exercise is who is in the wrong? Is it the druggist for using his monopoly power to deny a dying child access to life saving treatment? Is it us, as a desperate parent, who commits a burglary to save our child? Perhaps it’s our child who has the effrontery to create this situation by falling ill. Maybe it’s society as a whole for creating these impossible moral dilemmas in the first place.
I don’t remember how the class navigated the ethics of the problem. I think our solution was something along the lines of stealing the medication but repaying the druggist anonymously on the installment plan, it’s the kind of moral reasoning you find in college students. However, the whole thing came up to me again as I watch our society grapple with the impossible moral dilemmas we have created within our health care system. We, as a people, have spent decades allowing our health care system transform itself from a traditional service to a population into a behemoth of a big money industry and, with this transformation, we have created a whole series of problems that have been buried for far too long and which, like a cancer, continue to metastasize and sicken us all.
Every society that has ever existed, from Ancient Egypt, to medieval Europe, to the primitive tribes of the Amazonian jungle, has created a health care system. It’s part of our social DNA. As we gather in groups and form bonds of caring and community, some of us have always specialized as healers. Sickness, pain, injury, and other dis-eases are bound to strike and healers are those charged with interceding with the gods in order to restore balance to the body and harmony to the universe. Modern medicine retains vestiges of this priestly origin. Modern American doctors still wear ceremonial robes. We also carry ceremonial instruments of dubious utility. Those stethoscopes we carry are nowhere near as helpful as a chest x-ray and an echocardiogram. We also proffer healing magic in the form of a little slip of paper covered with incomprehensible script written in Medieval Latin known as a “prescription.”
I’ve always wondered about this god power myself. Over the third of a century that I’ve been in medicine I’ve had patients and their families look at me as if I’ve been imbued with some sort of supernatural substance when I have made a correct diagnosis or adjusted the medications in just the right way. I don’t get it. I know myself relatively well and I’m more Clark Kent than Superman. I struggled with this for a while until I fell back upon what I learned in high school and college about theater. When I understood that the white coat is a costume and ‘doctor’ is a role you inhabit, it got a bit easier. Some of us, however, forget to take the role off when we take the coat off and start to assume that we are something more. It can become a real problem when that attitude slops over into areas for which we were not trained… like politics.
The goal of these health care systems, no matter where you find them, has always been roughly the same, no matter the means they use to achieve them: get rid of dis-eases and by dis-ease I mean a whole plethora of things from infections to injuries to the physiologic changes of aging to the biological hazards of a normal condition such as pregnancy. The patterns are similar from Abyssinia to Zimbabwe. A previously healthy person becomes dis-eased and, when they reach the limit of their knowledge base or patience with the process, they turn to the healer to remove the problematic agent and restore balance and health. It’s been going on for the whole six thousand years of recorded human history and there is archeological evidence that it’s been going on for thousands of years before this. It leads to what we now call the acute care model of medicine. Something happens to me, I feel acutely ill and I depend upon the system to cure me, or at least make me better in some way.
For most of American history, the American health care system worked the same way. Actually, in the early years it wasn’t much of a system and didn’t work terribly well for anyone. In the colonial period and into the early republic, most health care was provided at home through family lore. A few physicians existed in cities for the treatment and comfort of the well heeled. The 19th century didn’t fare much better, with the majority of doctors self-styled through apprenticeships and dubious educational institutions.
The health care system, as we understand it now, started to coalesce in the period between the two world wars. For the most part, those with dis-eases were still cared for at home. The majority of physicians were general practitioners who cared for the community in which they lived. They had a consulting room, usually at their home and then made the rounds to check up on their patients in their Model T or mule cart, pulling up to mansions and hovels to do what was possible for the ill, instruct the families of the afflicted in proper nursing care and be a presence for comfort while nature took its course, one way or another. You could find some specialists in larger urban centers, gathered around money and the multispecialty clinic began to take form under models pioneered by the brothers Mayo in Rochester, Minnesota.
There were hospitals, but as medicine was a pay as you go cash business, most people tried to avoid them. In rural areas, especially during the depression when money was hard to come by, barter systems existed and the old trope of paying the doctor in chickens or a bushel of potatoes was born. This worked fine in communities where everyone knew everyone else but could not work in larger urban settings or with the local hospital board. Therefore, most hospitals had very narrowly defined mission. They were places capable of doing aseptic surgery, usually performed for life saving reasons such as the removal of a gangrenous gall bladder. They were places that could take care of people who did not have an intact family structure to provide nursing care during a period of dis-ease. They would protect communities by separating those who could be dangerous due to their potentially infectious state (the TB sanitarium) or because of erratic behavior (the asylum). They were small by current standards. Usually consisted of large open wards with minimal privacy, and were generally underfunded.
Medicine was a not for profit sector of the economy. Health care was regarded as a market good, but not one that people in general were interested in selling, as there wasn’t much money in it. Hospitals, descended from medieval religious institutions that tried to provide humane care for the poor and dis-eased following the example of Christ, were frequently chartered and run by religious organizations, especially Catholic, to provide a particular social good to the community. Those not run by religious organizations were usually publicly financed by cities, counties, states, and other governmental entities. Again, not for profit entities with specific social mission. The system here wasn’t that different than the system in the rest of the developed world. In fact, during the first third of the 20th century, it was far behind some of the great European centers of learning.
The first inklings of change, which would transform the US health system from its backward and bucolic roots, occurred in Dallas, Texas in 1929. At the time, Baylor hospital noted that the majority of their hospital beds were empty more often than not. The overhead of a nearly empty hospital was causing financial strain on the institution. At the time, the average American spent more on cosmetics than on health care (you tended to doctor yourself and your family with inexpensive over the counter remedies) and almost no families could afford a large hospital bill, so they were places to be avoided except in extreme circumstances. The fine folk who ran Baylor wanted to get their beds occupied by people who weren’t already at death’s door so they came up with the idea of having people buy health care in the same way they bought other consumer goods, a little bit at a time. They approached the Dallas teachers union with this idea. For an ongoing charge of fifty cents a month, members of the union could go to Baylor hospital for free.
Without necessarily intending to, they invented the modern concept of health insurance. Other hospitals saw value in this idea and started to offer similar deals, mainly to large groups of organized individuals such as unions and large employers. Eventually, these plans developed a new name, Blue Cross.
They spread throughout the country but most people didn’t buy into them until World War II upended the American economy. Wage and price controls left over from the Depression remained in place in the early 1940s just when the war fueled industrial machine required more and more workers to meet demand. Unable to offer higher salaries, large employers turned to fringe benefits to attract and retain workers. A court decision in 1943 declaring health benefits to be tax-free made medical insurance especially attractive to industry and this was further codified in the mid 50s at the behest of big business. By 1955, an employer based health system was here to stay. The rest of the industrialized world, recovering from the depredations of the war and the destruction of their infrastructures, did not move this direction. They needed a more cooperative model of health care leading to what Americans were decrying by the mid 1950s as socialized medicine. McCarthyism took a toll on American health care.
Many of us came of age during the period 1955-1980. We all remember health care as easy to obtain, Blue Cross being welcome everywhere, a stable family doctor who knew us well and who would both see us in the office or in the hospital if we happened to get ill. We carry that ideal around in our head as if that’s the way health care always was and always should be, rather than a unique time in a unique economy. At that time, our health care was the envy of the world, and we still carry the idea of American exceptionalism in medicine with us. Our hospitals were better, our doctors more knowledgeable, our research universities making exciting discoveries. The sparing of our society from the physical damage of World War II, our industrial capabilities allowing pharmaceuticals, especially antibiotics, to be mass produced, and our welcoming of the great medical scientists of Europe fleeing Nazi persecution, all led to us being the envy of the world.
Of course, this employer based system left certain groups out in the cold. Predominantly those who were post-employment, or retired. The Roosevelt administration toyed with adding health care to its New Deal social programs such as Social Security but there was a feeling that this was a bridge too far and with an increasing need to focus on the looming crisis of World War II, buried the idea. The Truman administration resurrected the idea of publicly funded health insurance for non-employed persons in the late 1940s but the rising tide of McCarthyism made any such social experiments suspect at best and communist at worst. The legislative language of the 1940s remained in draft form, and, when the political moment became right a generation later, the Johnson administration passed the Great Society programs including Medicare for elders, the disabled, and retirees and Medicaid for the impoverished, transforming the health care landscape in ways the original authors could not foresee.
Medicare and Medicaid were created to solve a particular problem. Non-employed populations had no access to hospital care. They couldn’t afford it. When they did turn up at a hospital, which was predominantly a not for profit institution established to provide a specific social good for either civic or religious reasons, it was the mission of the hospital to provide care first and ask questions about finances later. A generation of medical progress had taught the American population the ideal of American exceptionalism in medicine all too well and hospitals were rapidly transforming from the backwater of the health system to the shining centerpiece. It was also the hospitals that provided the muscle to push Medicare and Medicaid through a semi-recalcitrant congress, a battle reminiscent of today’s battles over health care legislation. Like all such battles, there was an equal and opposite reaction lobbying to maintain the status quo. In those days, that was represented by the AMA which viewed the programs as socialized medicine in another form and inherently bad for American Health. A massive propaganda campaign, led by an out of work B movie actor named Ronald Reagan, tried to change the path of the country and defeat the proposal but did not succeed.
The passage of Medicare, especially, was a huge success and there has rarely been a more popular social policy in American history. The elimination of large hospital bills through Medicare A and the significant reduction of outpatient expenses from Medicare B rapidly lifted the older generation out of medically induced poverty. It also opened the floodgates for federal dollars to start rushing through the health care sector of the economy, changing it within another generation from a relative backwater to a big business. The rules of the game in the immediate post war era, which defined health care as a social good that should be open to all, began to change.
The first major change was the introduction of the for profit company into health care. The profit motive was not new. Even in the good old days, doctors and hospitals tried to make money, but, having developed out of religious orders and civic institutions, nearly every organized piece of the system was not for profit. Moneys made were rolled back into the system in the form of improvements to facilities, new discoveries, or improved salaries for workers, not to pay dividends to shareholders. Laws required health insurance to be not for profit and all of the original Blue Cross companies of our youth were structured this way.
More and more money in the sector, however, did not go unnoticed by the financial sectors of our economic system. There had never been a lot of interest from Wall Street in health care in the past. The money was too small and the profits too slim, but billions from the federal government were a different matter and the system began to evolve. Bit by bit our country transformed our health care system into a health care industry. It began in earnest in 1973 when the Nixon administration, after personal lobbying of Nixon by his old friend industrialist Charles Kaiser, allowed health insurance companies and other health entities to operate as for profit businesses. Wall Street was ready and slowly, but steadily, the health economy moved from local control under a small business model to larger and larger corporations, often regional or national in nature. With these changes, a business mentality took over. Medicine stopped being about the individual and idiosyncratic dyad of healer and patient and became about the delivery of standardized product in the most efficient manner. With typical American ingenuity, our health care industry became more and more adept at this task in a for profit model.
As the health economy has grown and evolved over the last forty years, this process has accelerated and perfected itself. The healers are no longer in charge, the administrators are. They are the ones who speak the language of finance and big data sets and deliverables in an increasingly complex health care world and that’s what it’s all about. Like any mature industry, health care is now functioning in the United States exactly as designed. We still want to believe that it’s all about caring and compassion and making the lame to walk and the blind to see. It’s not. Our present health care industry is about what all modern industry is about – transferring the profits of that industry to the owners of that industry and it does that very, very well. So well in fact that it has become nigh on impossible to change the industry in any fundamental way. Any major change is likely to negatively impact the bottom line of various industry players and that cannot be allowed to happen despite the catastrophic fall of American health standards when ranked by the World Health Organization. Among developed nations, we’re dead last.
Among all nations, we’re 37th, right between Costa Rica and Slovenia. In some places, our child and maternal mortality statistics are worse than sub Saharan Africa. It’s not that American doctors are rotten or that we’ve lost knowledge and ability. People still flock from all over the world to our hospitals and to study in our medical research institutions. It’s just that we’ve changed the fundamental purpose of why we have health care from health to wealth and that no longer keeps wellness at the top of the reasons for it to exist, unlike nearly every other advanced world system.
Now I could go on for another half hour or so on specific flaws in our health care system and thinking such as our siloing of care by specialty, our overdependence on specialists, our refusal to accept death as a natural consequence of life, our training of the population to become creatures of pharmaceutical habit, and all the rest of the issues that many of us are familiar with but I’d rather bring this back closer to home and to who we are as UUs and why we spend our time with this religious community rather than one of the many other fine religious establishments in town.
Our first principle states that we affirm and promote the inherent dignity and worth of every person. The Universalist tradition comes from the idea of universal salvation. No one, but no one gets left out. To me, a church that ascribes to this worthy ideal must, by its very nature, ascribe to a health system that is similarly universal or it is vacating one of its core reasons for existence. We don’t have an everyone in system in this country but we have been cautiously moving that direction in recent decades and over the course of the last eight years, since the adoption of the Patient Protection and Affordable Care Act, a couple of very valuable things have happened. First, the number of people with access to the system increased enormously, more or less cutting the uninsured rate in half. Second, with access to health insurance, fewer health costs had to be borne by families and the rate of personal bankruptcy in the country has also fallen by half.
However, we now live in a different time. As a society, at least as far as our electoral choices reflect, we have firmly come down on the side of health care not being a right, but a privilege which should only be available to those with means. Our representatives in congress have been busy crafting legislation designed to enable the market forces behind health care to succeed at the expense of the people health care is supposed to serve. It doesn’t really matter whether you believe the congressional budget office, the department of health services, or industry trade groups regarding the projected outcomes. No one is predicting that any of the effects will do anything to make access to health care more just and equitable. At the moment, the ACHA in the house, the BRCA and the so-called skinny repeal in the senate appear to be dead, but with a political party having staked its reputation on changing a flawed system, I don’t believe for a minute that they’re going to stay dead. Especially in the reality television circus of current DC politics. The calculus of the Senate, in particular, is likely to change in markedly in 2018 and John McCain’s decisive no vote is subject to the vagaries of his own health needs.
The thing that bothers me the most about the current debate over health care is that it spends all of its time looking at how to cost shift from public sources of funding to individual and private sources of funding while spending no time at all looking at the reasons why our health care system is the most expensive in the world. The American health care system consumes 17% of our gross domestic product. In no other industrialized country is it more than 11% of GDP. With an American GDP of 18.5 trillion dollars, reducing our spending in line with other economies would give us about 1.1 trillion more dollars a year to spend on other needs. Or to improve and rebuild our health system until it is once again, the envy of the world.
The other thing that bothers me is a rather insidious change in the language and framing of the discussion of health care. It’s no longer a discussion of how can we help people, it’s now a discussion of who deserves to be helped. Every time I look at the news, I see an elected public official musing about the other, often in terms of ‘the cheaters’ or ‘the entitled’, especially when it comes to people on the lower end of the socioeconomic spectrum. I thought we had gotten rid of differentiating the deserving poor from the undeserving poor during the Victorian era when economists started to recognize that poverty was usually the result of macroeconomic forces and not due to personal choices. Sober minded individuals, usually affluent white men, proffer rhetoric of ‘three strikes and you’re out’ in terms of life saving treatments, suggest that no access to health insurance is fine because there are always emergency rooms (showing a fundamental misunderstanding of how the health system works), or speak of millions of children and elderly being thrown off of Medicaid rolls as a good thing. In most states between a third and a half of children rely on Medicaid for health care. With major cuts, some of those children will die. Let’s call it what it is. Human sacrifice.
The idea of asking Americans to take responsibility for their own health rather than just assume that the health system will care for them is a laudable one but it’s not as easy as it seems. Imposing it from the top in a punitive way through fines or increased costs is only likely to drive people away from the system leading to disease being found later, at a more advanced stage and ultimately driving up costs. For it to work, we have to attack health literacy on a societal level. Starting early in life, people have to be taught how their bodies work and have to be taught that health is a partnership with a healer, not something that is done to them. This, of course will require a much more robust primary care system than we have in this country. We know how to build such a system but to do so, you have to have about three quarters of your physicians in primary care and one quarter in specialty care. The United States has the opposite proportions. It will also require more scrupulous honesty in American society about the naturalness and necessity of death (a whole sermon unto itself) and an understanding that a system that tries to cover all possible treatments for all people all of the time is doomed to failure and that certain types of choices must be made and should be approached with science and rationality – both qualities currently missing from the American political system.
There is a huge problem with placing personal value judgments on health care and patients. It’s a lesson I learned early on in my medical training. I was a medical student in the mid 1980s at the height of the HIV epidemic. People were dying of a preventable disease due to our society and government’s unwillingness to understand marginalized populations. One day while on the internal medicine service, our team was caring for two HIV patients. One was a young man in his late teens or early twenties, the other a grandmotherly woman of sixty or so. The young man was about as fey as they come. You could have seen the flames coming off him from space. His effeminate mannerisms were a kind of psychic armor helping him cope with the fact that he was unlikely to live to twenty-five. The older woman was the sort of woman you expected to bring you milk and cookies and tell you about your day while she knitted you some new wooly socks. My attending physician, a well-known internist in his fifties ended our rounds and walked away with the comment. “You know, it’s too bad that poor woman is an innocent victim of AIDS but that guy deserves it”. I was a little more familiar with the patients than he was. The young man was a hemophiliac who contracted it through his need for transfusions. He had never had a sexual relationship in his life and probably never would. The older woman was a swinger. Value judgments are a very slippery slope, which is why the Hippocratic Oath has read as it does for three thousand years. And, no matter how you slice it, no one ‘deserves’ disease.
Where does this leave us? To tell you the truth, I don’t know. I’m just one small individual in a stormy sea of a system that’s gone somewhat off the rails. I don’t have the power to fix it. All I can do is what I have always done, save the world one patient as a time. There’s an old Chinese proverb, some say a curse. ‘May you live in interesting times’. Well, these are interesting times and the health care system, which has always been a bit of a wild ride, is bound to get wilder. Hang on and fasten your seat belts.