It’s only been three days since the last one of these entries but it seems like several months have gone by in the interim. Something seems to have happened to my perception of time. It feels normal in the immediate here and now but once something slips into the past, it’s as if there’s a great acceleration. Perhaps its the dizzying pace of events as the country reels from political and public health upheavals. Perhaps this is what happens when you age. My patients have always talked about time moving so quickly in their later years. It’s just that if feels like the inauguration was three months ago rather than three days ago. Or maybe it’s the rapid proliferation of 10,000 Bernie Sanders mittens memes…
With a new administration in place. things are beginning to change for the better in terms of the federal response to the corona virus pandemic. The administration has released its plan for bringing the plague under control and its a common sense compendium of tried and true public health measures, most of which should have been in place last spring. It has taken the availability of vaccines into account and there are now federal plans to utilize the national guard and other elements of the government to get vaccine out as quickly as it can be manufactured.
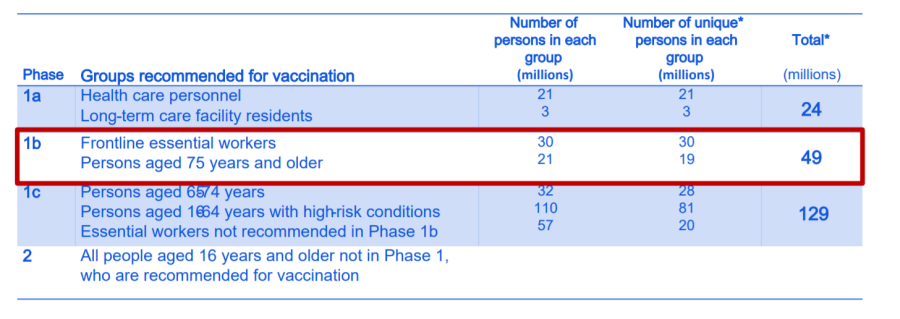
Locally, we here in Alabama are stymied by shortages in vaccine supply. The Alabama Department of Public Health who controls all distribution in the state has gotten its act together and is getting vaccine out to various points to begin vaccinating those over age 75, however, the complete lack of federal coordination has kept vaccine from flowing into the state to meet demand. Vaccinators often don’t know when they are going to get a shipment until a few hours before it arrives which makes setting up schedules and notifying patients a wee bit difficult. There are plans for several mass vaccination sites in the greater Birmingham area and the logistics are in place but they can’t open them up until there is a supply that can be counted on for both first and second shots.
In the meantime, numbers continue to mushroom. There is some evidence that we have peaked and we may be on the downward side of the hump caused by holiday gatherings and travel from Halloween through New Years. Numbers in the hospital locally are down slightly. The percentage of positive tests is decreasing somewhat (but is still more than double the five percent which is thought to be the level at which we can consider the pandemic under control in a particular area). Anthony Fauci has finally been allowed to share his expertise with the public untrammelled and is now responsive only to science and not to politics and his expression of delight at being able to at long last speak unvarnished truth and swing the CDC and other health organizations toward protecting the public rather than protecting the optics of the White House has been rather refreshing. The next big issue is the spreading of the UK variant which is significantly more contagious than the original strains. If this isn’t slowed, we may barely get a rest from this peak before a whole other surge begins later this spring.

Tonight was the one year anniversary of the opening of the Virginia Samford Theater’s production of Cabaret, the last live stage show I was part of during the ‘before’ times. The cast gathered on zoom to toast each other and watch an archival video of a performance together. I don’t like watching myself in such things – stage perforrmances depend so much on the interaction of the actors with the audience that you always feel removed on both sides of the equation when it’s on screen. However, it was fun to see everyone and to reminisce and to comment on how appropriate that piece was to the political times we have been living in recently. When the local theater world opens back up, we’re going to lobby for the theater to revive that production. One year later and I’ve just started rehearsal on another theater project, a zoom theater version of Tartuffe in which I am playing Orgon. Now there’s another play that’s perfectly in synch with the current political times despite being four hundred years old. That’s what makes great art, something born out of turbulent times that helps a future generation understand the turbulent times in which it finds itself.
Bad times, pandemic disease, political unrest, religious schism – no society is immune from such things. We like to think of ourselves as privileged individuals living in the finest civilization the world has produced, an apogee of comfort and enlightenment. I’m pretty sure the Ancient Sumerians, the Imperial Romans, Tudor British, 18th century French, and all the others felt the same way about themselves and their societies in their day. I think it’s part of the human condition to believe it can’t happen here until it does.
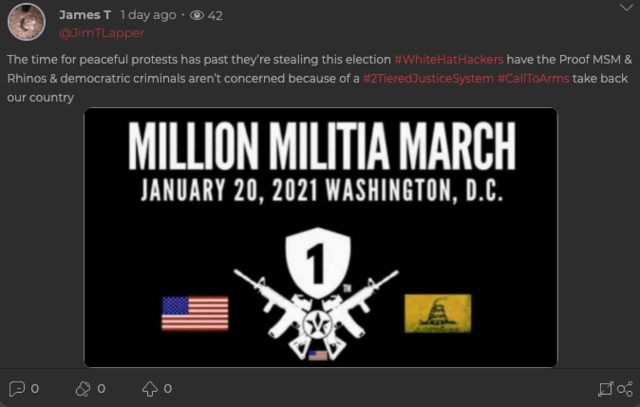
I have no idea how the new administration is going to go about solving the myriad problems in American society that our failed response to the corona virus has exposed. I don’t know what the opposition to President Biden and the Democratic party has planned in terms of response. All I can say is that there’s going to be no linking arms around the campfire and singing Kumbyah. We’re a long way from controlling this pandemic and we must all continue to be vigilant, vaccinated or not. Hundreds of thousands have died, hundreds of thousands more are likely to die but we can each do our own small part to protect each other. You all know what to do. Stay home, wash your hands, wear your masks and social distance.